Rashmi Rao: Gender Health Gap: Why Isn’t She the Default?
May 30, 2025


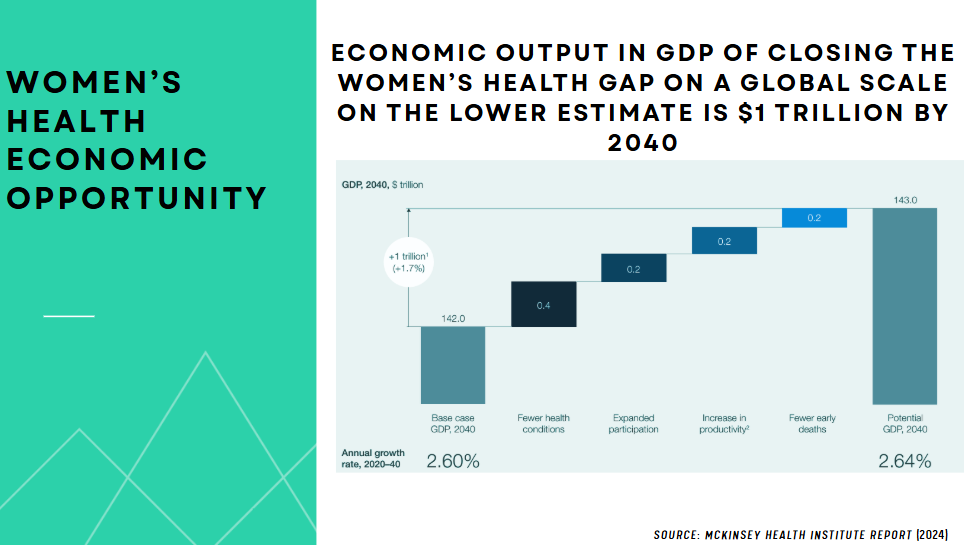
Even as global life expectancy has risen dramatically — from 30 years in 1800 to over 73 today — women’s “healthspan” has stagnated. Women spend 25% more time in poor health than men. That gap is global. According to the McKinsey Health Institute, closing this gendered health gap could unlock $1 trillion in annual global economic gains by 2040. Yet healthcare systems, research agendas, and funding flows continue to center male biology as the default — treating women as exceptions.
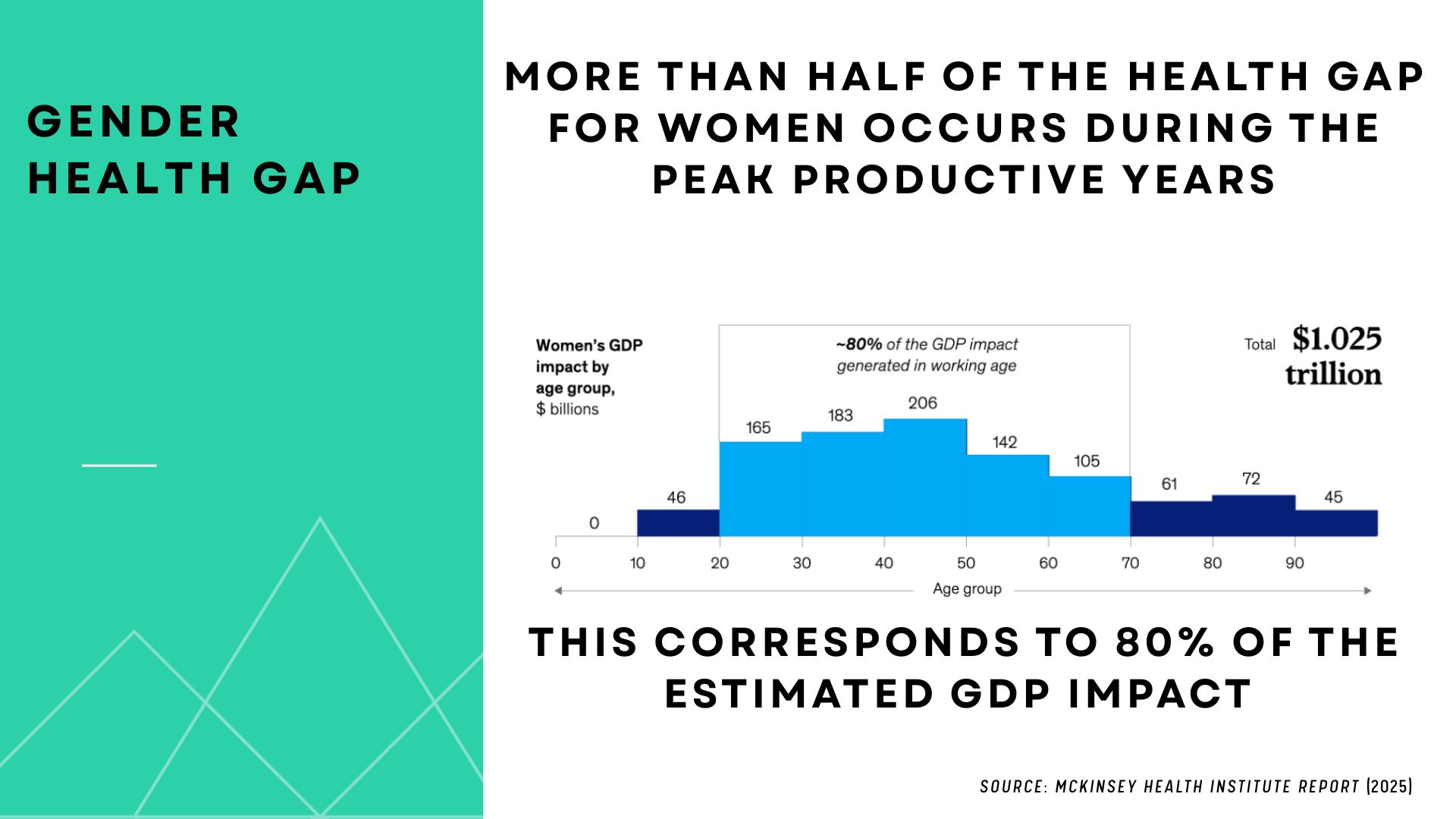
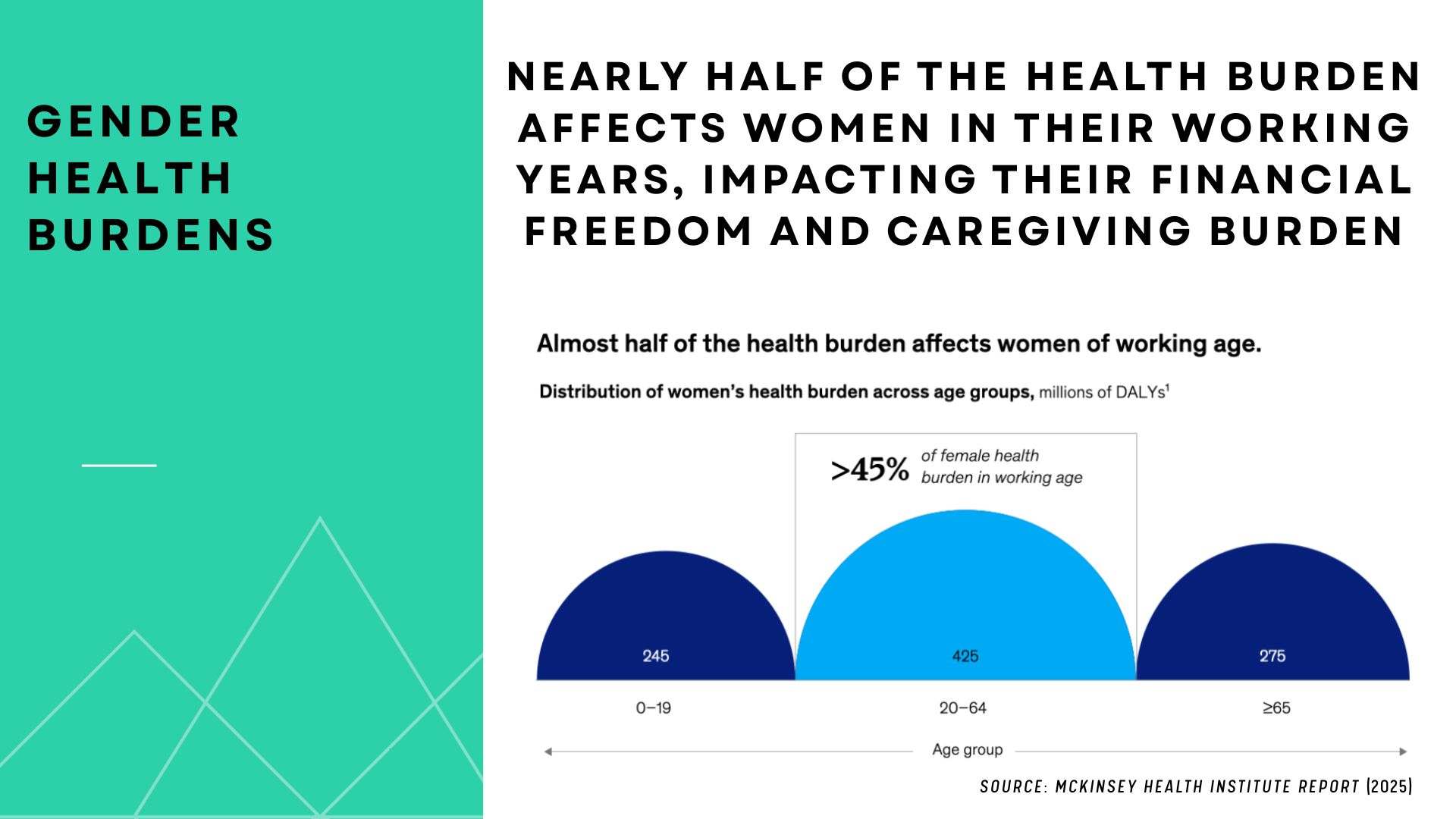
Women live longer, but not better. Most of the health burden occurs during their most productive years, impacting workforce participation, caregiving roles, and long-term economic stability.
Beyond Reproductive Health: Reframing the Narrative
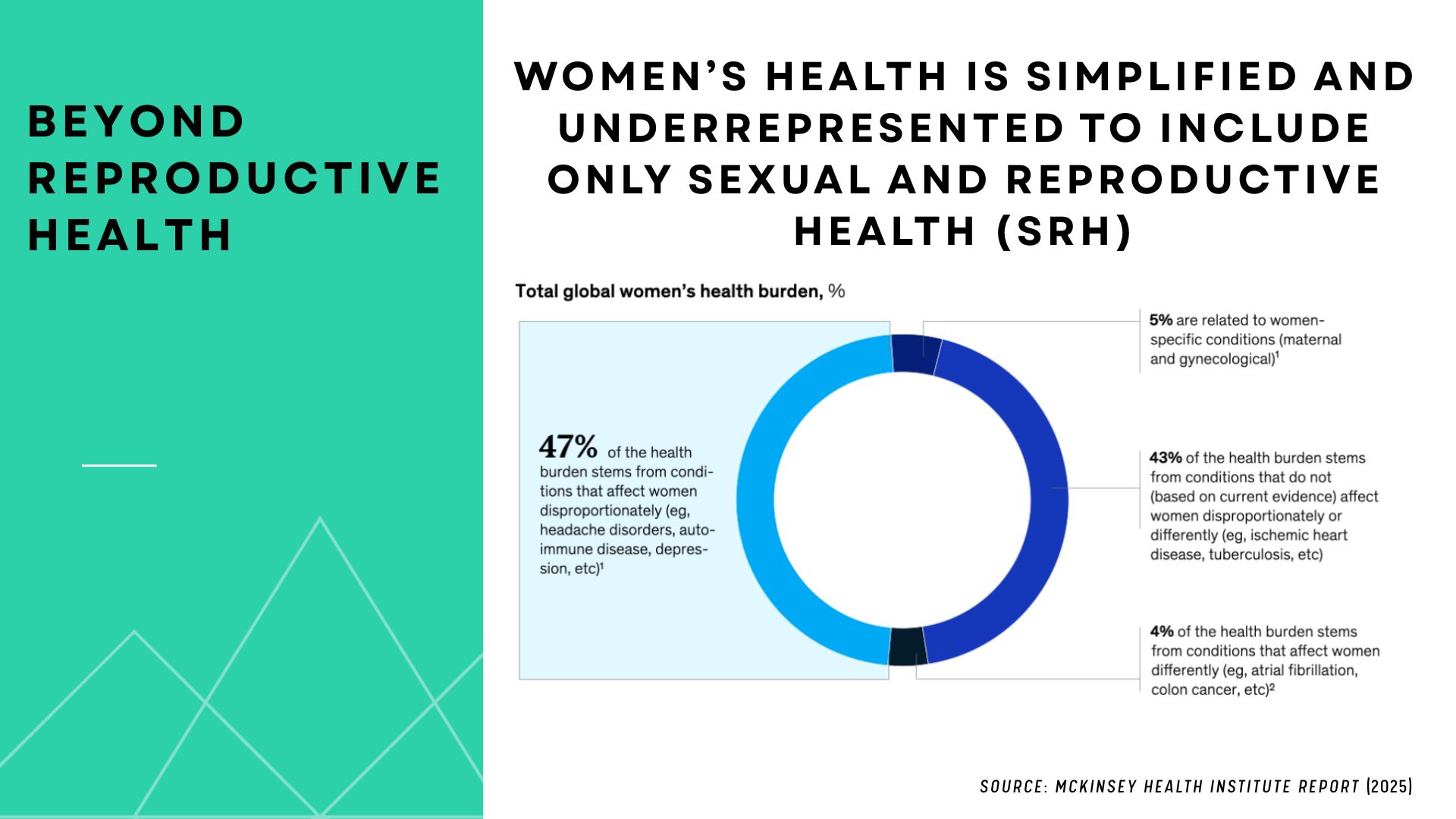
Women’s health has too often been reduced to sexual and reproductive care. But maternal health makes up only 5% of the total burden of women’s health issues. The real drivers? heart disease, autoimmune disorders, mental health, perimenopause, caregiving-related stress and systemic neglect.
As the Springboard and Accenture report emphasizes, women’s health has been consistently underfunded, under-researched, and misunderstood — with female-dominant diseases 8x more likely to be underfunded by NIH than male-dominant ones.
This isn’t a “niche market.” It’s half the population — who also make 82% of healthcare decisions in our families and communities and give birth to 100% of the next generation.
Conditions Driving the Gender Health Gap
More than a third of the global gender health gap stems from just ten conditions — some impacting how long women live, others affecting how well they live. Understanding these conditions is essential for setting priorities in research, funding, and care. How severely they impact women’s health — whether through early mortality or years lived in pain — varies widely based on race, income, geography, and access to care. That’s why addressing them requires not only medical intervention but systemic, equity-driven solutions.
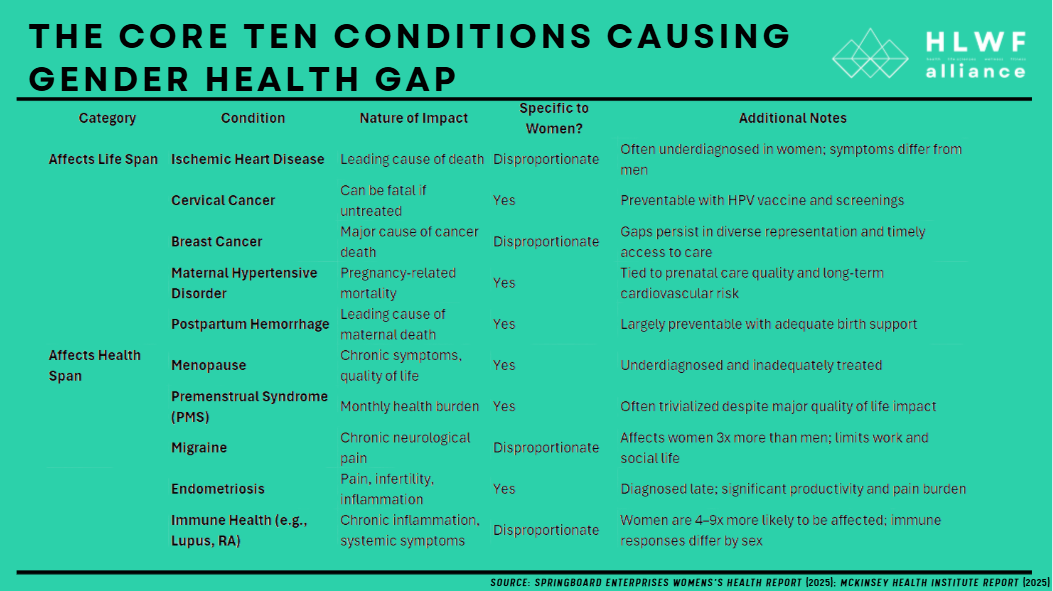
We now know that women are more likely to suffer adverse drug reactions, experience diagnostic delays, and die from heart conditions because clinical trials, regulatory frameworks, and innovation systems were built without them in mind. Women represent 80% of autoimmune disease patients, yet only 7% of NIH-sponsored autoimmune research focuses on them.
Menopause — affecting 50 million women in the U.S. — is still treated like a footnote. Yet it intersects with heart disease, brain health, and workplace readiness, especially for women in the military and beyond. Heart disease is the #1 killer of postmenopausal women, but only 4.5% of coronary research targets their needs. Recognizing its impact through mandated defense reporting would improve not just health outcomes, but national performance and workforce retention.
Addressing Gender Health Gap:
The core elements of the gender health gap indicate a need for better data, more effective interventions, improved care delivery, including all genders equitably, and increased investment in women specific health research and solutions.
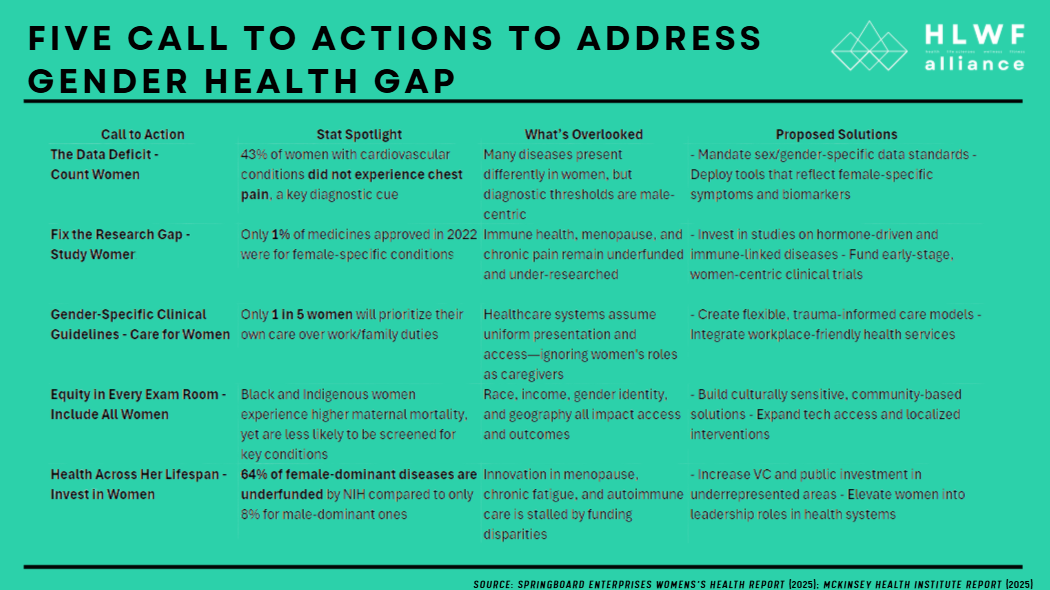
A targeted investment of just $200 million across NIH institutes for coordinated, sex-based data collection and interdisciplinary women’s health research could radically improve care and drive innovation. Meanwhile, establishing a $5 million FDA Women’s Health Innovation Program would accelerate life-saving solutions to market, informed by the very biology they intend to serve. The economic return? Up to $14 billion, just by doubling current NIH spending in key areas like heart, brain, and immune health. The path forward requires systemic change — not just new treatments. Based on leading insights from McKinsey and Springboard, these five calls to action offer a blueprint for transformation.
1. The Data Deficit: Count Women
The problem: Women weren’t required in NIH-funded clinical research until 1993. Today, their experiences still get sidelined in health data, leading to delayed diagnoses and inappropriate treatments.
Most medical research still centers male physiology. In cardiovascular care alone, symptoms like chest “tightness” or nausea in women are overlooked because diagnostic models are based on men.

Further, key subpopulations such as women of color and post-menopausal women remain under-represented in clinical trials. Only 5% of available
medications have been adequately monitored, tested and labelled with safety information for use in pregnant and breastfeeding women.
What’s missing? Data that reflects real, diverse women’s lives — across life stage, race, age, geography, and identity.
Action needed:
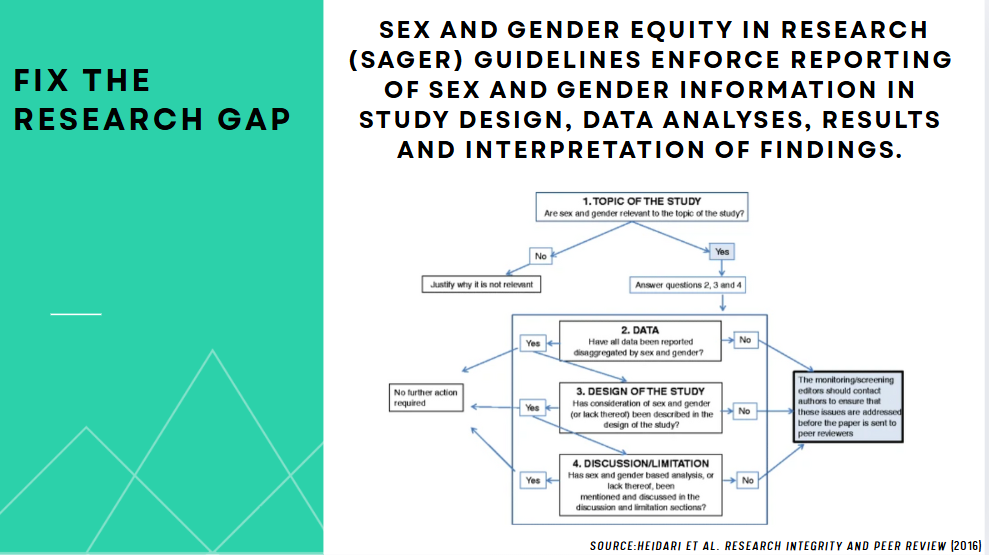
2. Fix the Research Gap: Study Women
The problem: Diseases that disproportionately affect women — like endometriosis, autoimmune disorders, and perimenopause — are severely under-researched. Funding lags far behind need.
In 2023, women’s health startups received only $1.1 billion of $26.5 billion in healthcare venture capital. That’s just 4%.
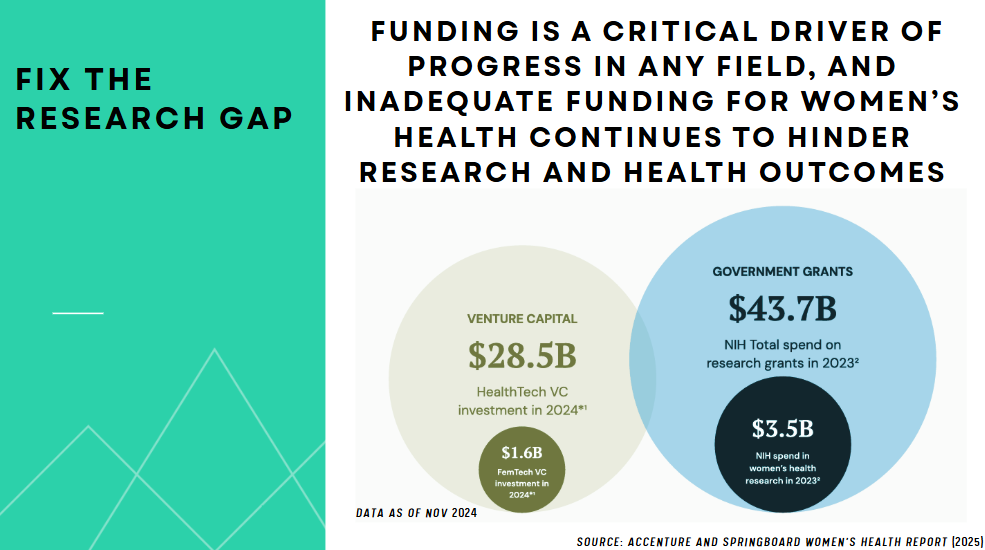
Why does this matter? Lack of research means lack of innovation. It also means poor reimbursement, fewer clinical guidelines, and lives in limbo.
Solutions:
Bottom line: Women are not just “small men.” They deserve research that reflects their biology.
3. Center Gender-Specific Clinical Guidelines: Care for Women
The problem: Most care models are one-size-fits-men. Clinical guidelines fail to account for sex-based differences in symptoms, medication response, and treatment efficacy. For example — Women are more likely to be misdiagnosed for heart attacks. Men are more likely to be referred for surgery, even when symptoms are identical.
Why does this matter? Women physicians deliver better outcomes — but are reimbursed less. In similar procedures, male-dominated specialties like urology get higher compensation than OB-GYNs, even for longer, more complex procedures.
Solutions:
What this means for systems: A holistic, gender-aware approach reduces long-term costs and improves outcomes for everyone — not just women.
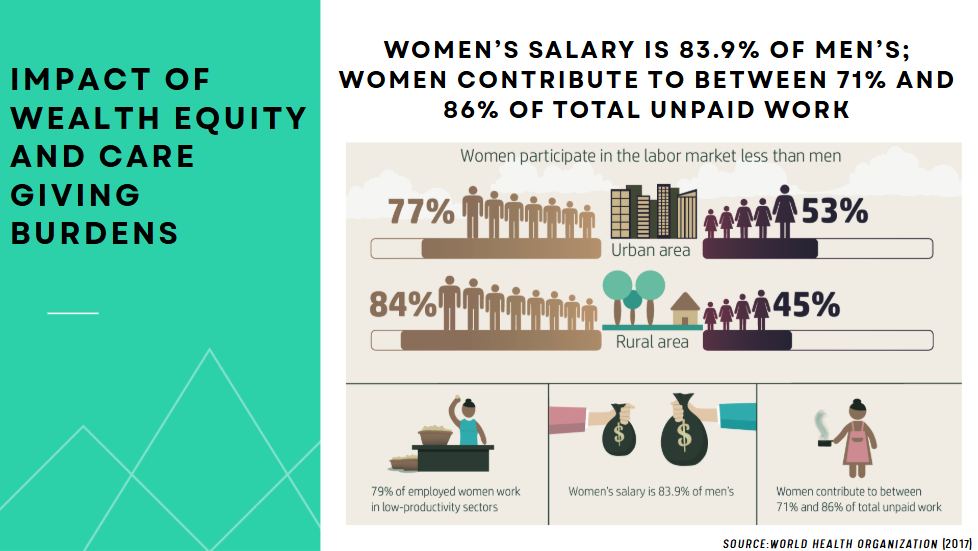
4. Equity in Every Exam Room — Include All Women
The problem: Not all women are equally seen — or served. Low-income women, women of color, LGBTQ+ women, and single mothers face compounding barriers to care.
Nearly half of all women’s health burdens occur during working years, affecting career trajectory, financial stability, and mental health. Yet systems aren’t built to accommodate that complexity.
Lived experience: Women with trauma histories, environmental stress, or caregiving obligations often go without care — not because they don’t want help, but because systems weren’t designed for them.
Solutions:
Provocative idea: What if companies treated employee caregiving the way they treat community service? What if wellness started at work?
5. Health Across Her Lifespan — Invest in Women
The problem: Investment in women’s health is reactive, not proactive. Most funding focuses on reproductive years — leaving out childhood, menopause, and aging.
A $300 million investment in women-centric R&D could generate $13 billion in savings through productivity and reduced health costs.
Women’s economic participation has been and will be a major driver of economic growth since the 1950s. Addressing the gap could generate the equivalent impact of 137 million women accessing full-time positions by 2040.
What’s overlooked?
Solutions:
This isn’t a handout. It’s a smart investment — with exponential returns.
Let’s Rewrite the Default
Women’s health is generational health. Women’s health is the future of our species and the future of our planet. Women’s health isn’t niche. It isn’t optional. And it definitely isn’t just about reproduction.
It’s about whether women are believed when they’re in pain. It’s about data, reimbursement, equity, and policy. It’s about whether half the population is seen, studied, and served.
So, why isn’t she the default?
Because too often, systems weren’t built with her in mind. But now we know better. We have the data. We have the voices. We have the urgency.
Let’s make “her” the default — not just in medicine, but in research, investment, and care.
The future of health depends on it.
REFERENCES:
Rashmi R. Rao , Managing Director, rcubed | ventures; Founder / Board Chair, HLWF℠ Alliance
“There is never a bad day to have a good idea”, is what you would hear Ms. Rashmi Rao say often.
Ms. Rao is an entrepreneur and inventor with 40+ patents and demonstrated prowess in transforming ideas to lucrative tech and healthcare businesses generating $500M+ revenue at Apple, Samsung, Qualcomm, and Philips Healthcare. Rashmi was inducted into the Top100 Health tech Women leaders (2024, 2025) and the Women in Tech Hall of Fame (2018) and has over 40+ granted patents. Rashmi has scaled and exited three companies and built and managed teams of up to 350+ people globally and has an impressive track record in managing venture funds, overseeing successful exits and participating in notable acquisitions. At Philips Healthcare, Rashmi spearheaded AI-powered consumer health solutions and secured a $500M insurance contract. She led the development of off-line AI models and integration with Apple HealthKit, which generated $150M+ in annual revenue. In Apr 2025, Rashmi published a book on AI in Healthcare with a specific focus on the US and Global Regulatory landscape for AI applications in Healthcare. As the Founder of rcubed | ventures, Rashmi invests in startups focused on value-based care, remote monitoring, and sustainability, leveraging her healthcare and M&A expertise. She also leads HLWF℠ Alliance, a non-profit dedicated to breaking silos in healthcare, health tech, and life sciences to tackle systemic health inequities. Rashmi is well-recognized for her board expertise and serves on the board of World Affairs Council, and University of Washington, Engineering Innovation in Health (EIH) to lend her expertise at the intersections of social innovation, public health and public policy. She resides in Sammamish, WA, with her spouse and two sons.